Poor mental and physical health of employees is associated with premature labour market exit, higher sickness absence and presenteeism. This in turn contributes to lost productivity and lower employee retention. Poor health often starts early in working careers and the effects can accumulate over time. Managing a multigenerational workforce requires employers to think intentionally about how the workplace they create promotes good health of workers at all ages. This chapter highlights employer and government policies that can contribute to healthier workers and workplaces.
Retaining Talent at All Ages
Ageing and Employment Policies
3. Staying healthy with age: Promoting healthy ageing in the workplace
Abstract
Key messages
Ill-health results in lost productivity and higher turnover through absence and presenteeism and is a major driver for premature labour market exit among mature workers
In 2019, around 20% of workers aged 35-44 voluntarily left their jobs because of poor health, and this share was higher (25%) among workers aged 50-64.
Results from the 2022 AARP Global Employee Survey shows that health problems were a reason for retiring early for 25% of workers aged 55‑64.
Job strain, stress and burnout affects almost one in every three employees in OECD countries.
On average among 25 European OECD countries the sickness absence rate is 1.3% among young workers, 2% among prime aged workers, and 3.2% among mature workers.
Greater efforts to tackle health at the workplace will be key to prevent talent loss
Comprehensive and integrated workplace health or well-being programmes can improve health, productivity and retention.
Governments and social partners can support small and medium enterprises (SMEs) in implementing workplace health and well-being programmes by strengthening occupational health services, developing national accreditation for health and well-being providers, and by creating certified recognition programmes for employers.
Workplace accommodation and job redesign are essential tools to retain workers with ill health. Improving employee control over work, reducing excessive work demands and enhancing social relationships at work can improve health and well-being.
Paid sick leave can play a key role in promoting better health by allowing sick workers to recover at home and ensuring they can access medical support. However, this must be accompanied by active return-to-work measures to prevent avoidable long-term absence which can be costly for employers, the workers concerned and society.
Employee attachment to employers can be maintained following illness by using gradual return to work schemes, where necessary, and by making accommodations for workers with health conditions. This can prevent the loss of skills and experience, and in some cases the partial return to work can help with rehabilitation.
With the rise of teleworking following the COVID‑19 pandemic, governments and employers have a key role to play in mitigating any negative impact on mental health impact. For example, some countries now have legislation in place giving workers the right to digitally disconnect outside of standard working hours.
3.1. Poor health is a key driver of employee turnover and absence
The negative effects of poor working conditions on employee health (Box 3.1) take their toll on workplace outcomes such as employee turnover, absence, presenteeism, premature labour market exit and productivity. Poor health is a key driver of labour market turnover. In 2019, 20% of workers aged 35‑44 and 25% of workers aged 50-64 left their current job because of ill-health (Chapter 1, Figure 1.12). People with poor health are less likely to be employed and face greater labour market disadvantage generally. Once employed, people with poor health are also less likely to remain in employment compared to people in good health (Webber et al., 2015[1]).
The two most common groups of health problems are musculoskeletal disorders (MSDs) and common mental health problems such as depression and anxiety. Because of population ageing and greater longevity there will be an increasing proportion of older workers in the workforce, who are twice as likely as 35‑54 year‑olds to have multiple long-term conditions including physical and mental health (OECD, 2020[2]). Older workers are therefore more likely to change jobs, change the type of work they are doing, or leave the labour market altogether. Poor health also varies by other socio‑economic characteristics, in all OECD countries with available data, older people in the lowest quintile of the income distribution are more likely to be in poor health than those in the highest quintile (OECD, 2021[3]). Employers therefore need to support all employees regardless of age or life stage if they have long-term or chronic conditions which may limit their ability to perform effectively at work and retain them at the workplace.
Box 3.1. Poor quality jobs can cause poor health
Poor quality jobs harm the mental and physical health of employees (Marmot and Smith, 1997[4]; Marmot et al., 2020[5]; Cottini and Lucifora, 2013[6]). One measure of a poor quality working environment is job strain, experienced by almost one‑third of employees in OECD countries in 2015, and defined as a situation where the job demands experienced by workers (i.e. physical demands, work intensity, inflexible working hours) exceed the resources available to them (i.e. task discretion, training, career advancement) (Cazes, Hijzen and Saint-Martin, 2015[7]). The share of employees experiencing job strain is generally higher in central and southern European countries (peaking at almost 50% in Greece), while affecting around 20% of employees in northern Europe and New Zealand (Figure 3.1). Individuals exposed to high levels of job strain are more likely to develop cardiovascular and coronary heart disease, hypertension, musculoskeletal disorders and high blood pressure from work accidents (Saint-Martin, Inanc and Prinz, 2018[8]).
Figure 3.1. Job strain affects almost one in every three employees in OECD countries
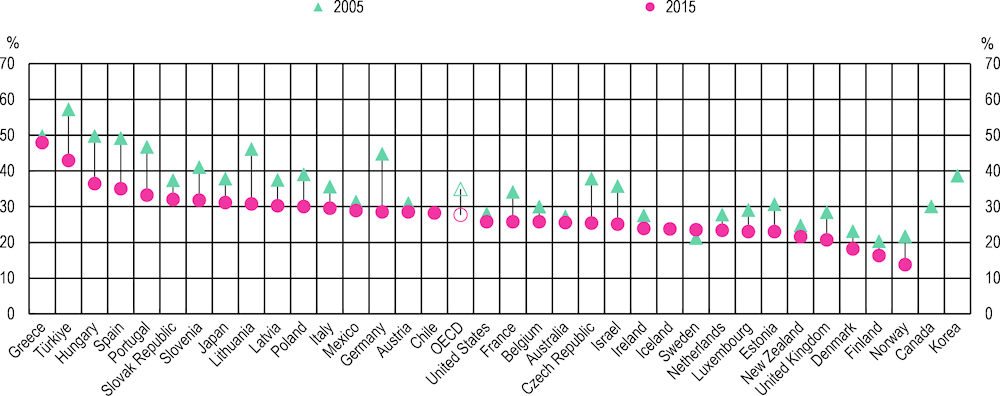
Note: OECD is the unweighted average of 31 countries and excludes Canada, Chile, Colombia, Costa Rica, Iceland, Korea and Switzerland due to incomplete time series.
Source: OECD Job Quality Database, http://stats.oecd.org/Index.aspx?DataSetCode=JOBQ.
3.1.1. The costs of absence and presenteeism are large
Absence from work because of sickness reduces the productive capacity of an organisation and can often be a way in which workers end up leaving the labour market altogether. The absence of one employee can also lead to declines in the productivity of remaining workers, as the co-workers are asked to “fill in the gaps” and compensate. The indirect costs of illness or injury (productivity) then add up to roughly the same if not more than the direct costs (hospital stay and medication), effectively doubling the total cost of sickness absence (McNamara and Tinsley-Fix, 2018[9]).
The prevalence of sickness absence various substantially across countries. On average among 25 European OECD countries the sickness absence rate is 1.3% among young workers, 2% among prime aged workers, and 3.2% among mature1 workers (Figure 3.2). In Belgium, Portugal, Norway, Germany, Spain the rate for mature workers is at or above 5%, and rates for prime‑aged workers are 3% or more in Norway, France, Belgium, Portugal, Germany and Slovenia.
Figure 3.2. Older workers are more likely to experience sickness absence for health reasons
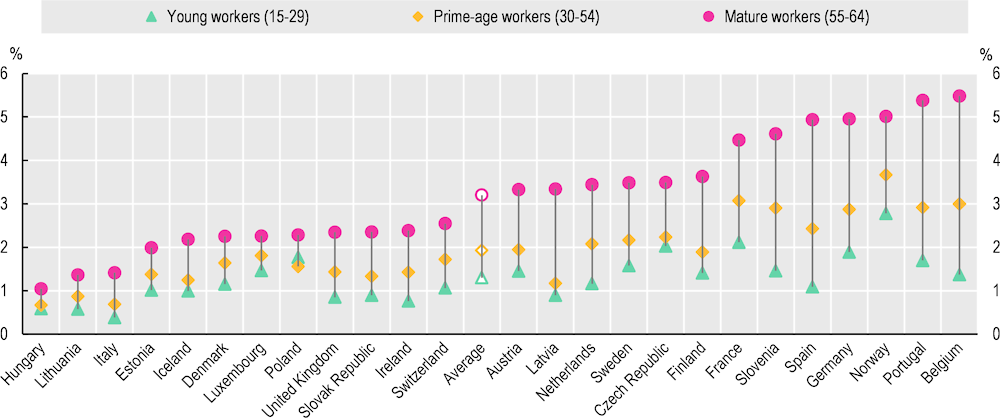
Note: The unfilled markers represent the average of the 25 countries shown. Derived from the variable ‘nowkreas’ (reason for not having worked at all during the reference week though having a job), and the response “Own illness, injury or temporary disability”. The denominator is total employment.
Source: OECD calculations based on the European Union Labour Force Survey (EU-LFS).
While the costs of sickness absence may be large, the cost of presenteeism – the lost productivity of attending work when unwell – is estimated to be 1.5 times higher than sickness absence (OECD, 2020[2]). The latest data suggest that employees in France, Denmark and the United Kingdom have the highest rate of presenteeism in European OECD countries (Figure 3.3). There is a risk that employers may underestimate employee ill health by focusing solely on absence. Evidence from the study of the long-term health of UK Civil Servants (Whitehall II) shows, presenteeism may be detrimental to employee health in the long run because it can “mask” serious illness (Marmot et al., 2010[10]).
Poor mental health also increases the prevalence of sickness absence and workers with poor mental health (for example depression or anxiety) are likely to be far less productive even when at work (OECD, 2012[11]). There is often a stigma associated with mental health issues such that presenteeism is likely to be common (OECD, 2021[12]).
Figure 3.3. Self-reported presenteeism in the EU, 2010 and 2015
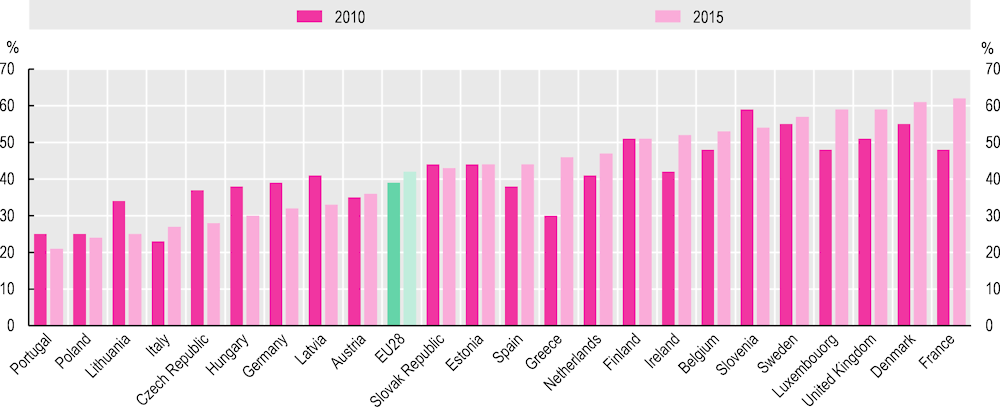
Note: EU28 is a weighted average.
Source: OECD (2020[2]), Promoting an Age‑Inclusive Workforce: Living, Learning and Earning Longer, https://doi.org/10.1787/59752153-en, Figure 4.7.
3.1.2. Loss of talent through premature labour market exit
Ill health, unresolved or long-term sickness absence can lead to early retirement or premature labour market exit, i.e. leaving before the state pension age. For instance, results from the 2022 AARP Global Employee Survey shows that health problems were a reason for retiring early for 25% of workers aged 55‑64 (Chapter 1, Figure 1.13). Further evidence suggests that that since COVID-19, ill-health may have contributed to surge in activity among older workers in some OECD countries such as the United Kingdom (Haskel and Martin, 2022[13]).
Data from other indicators, such as effective retirement ages shows that although statutory retirement ages have risen, people still leave well before state pension age. In all OECD countries, despite the significant increases in life expectancy, the effective retirement age is still lower today than it was 30 years ago (OECD, 2022[14]). Although institutional factors such as the availability of early pension benefits, difficult working conditions and caregiving responsibilities play a role, poor health is also important (OECD, 2018[15]).
Disability is another channel through which workers may leave their jobs and can prevent people gaining employment at all ages. Among those who do, or who develop conditions later in life, exiting the labour market permanently due to disability is all too common. While not all workers with disability have the capacity to work, evidence suggest that many are often still able and want to continue working provided the right support and conditions are provided (OECD, 2022[16]).2
Similarly, disability due to mental health conditions is strongly associated with lower employment. Moreover, many individuals with mental health conditions are unable to find or keep jobs. On average, across OECD countries, 60% of people with moderate mental health conditions are employed compared to 70% of those without a mental health condition (OECD, 2021[12]). Individuals with a mental health condition are also almost twice as likely (85% higher) to be unemployed, indicating that many are either looking for jobs without success and/or are transitioning into and out of work more often (OECD, 2021[12]). The COVID-19 pandemic has led to major changes in working arrangements for many people, such as increased teleworking. While there are benefits such as increased flexibility associated with this, there are also potential negative consequences for mental and emotional wellbeing if remote work is not carefully managed (Bevan and Cooper, 2022[17]).
Overall, as the number of working age people with long-term health conditions rises, Government and employers need to improve workplaces and support systems to help people to manage their health conditions and remain at work.
3.2. Promoting health and well-being in the workplace
Preventing ill-health starts from childhood through preventing obesity, smoking, harmful use of alcohol, and sedentary lifestyles, for example. It is critical to support policies to prevent ill-health throughout employment as the effects of poor health can accumulate over time. With an ageing workforce, both employers and governments play a key role in ensuring the good health and well-being of the workforce.
3.2.1. Workplace health and well-being programmes can improve worker productivity and well-being
Workplace health and well-being programmes (WHWP) are employer driven initiatives directed at improving the health and well-being of workers. This can include programmes that encourage exercise, healthy eating, stress management, smoking cessation, as well as interventions aimed at ailments such as diabetes, cardiovascular diseases (CVDs), musculoskeletal disorders, and depression. Many companies are also providing broader programmes that blend a range of physical, social/emotional, and financial programmes (OECD, 2020[2]). Financial security programmes are increasingly common, as it is recognised that it is difficult to engage employee’s wider health needs if they are struggling with managing a budget or large household debts.
Evidence on the effectiveness of WHWP is mixed. Recent meta-reviews of WHWP suggest that programmes can (on average) reduce medical costs, and improve health and productivity (Baicker, Cutler and Song, 2010[18]; Baxter et al., 2014[19]; Chapman, 2012[20]; Mattke et al., 2013[21]). However, these reviews find that the effects of health programmes vary depending on the type of evaluation method used. Because healthier people are more likely to participate in workplace health programmes, robust evaluation using randomised experimental methods is necessary to gauge whether a programme has a positive effect. Habits about diet and exercise are often deeply rooted and not easily amenable to change; often people respond to financial incentives in the short term but fall back into old patterns once the incentives end (Royer, Stehr and Sydnor, 2015[22]). Overall evidence suggests that ‘medicalised’ interventions to improve exercise or diet, for example, are less successful than holistic interventions which focus on organisational climate, job quality, job design, flexible working, social support, and matching resources to job demands (Bevan and Cooper, 2022[17]).
Meta-reviews also show that the comprehensiveness, intensity and duration of WHWP varies widely.3 Further research is still needed to fully understand which attributes of health programmes are the most important and how such programmes should be optimally designed. Nevertheless, existing evidence points to elements of promising practices (Goetzel and Ozminkowski, 2008[23]). These are: a) integrating programmes into the organisation’s central operations; b) addressing individual, environmental, policy, and cultural factors affecting health and productivity; c) targeting several health issues simultaneously; d) tailoring programmes to address specific needs of the population; e) attaining high participation rates; f) rigorously evaluating outcomes; and g) effectively communicating these outcomes to key stakeholders (Goetzel and Ozminkowski, 2008[23]). The Centers for Disease Control and Prevention (CDC) also emphasise the importance of a co‑ordinated, comprehensive set of programmes, policies, benefits and environmental supports for a successful workplace health programme (Centers for Disease Control and Prevention, 2016[24]). The workplace health programmes in Box 3.2 illustrate many of these features.
Box 3.2. Workplace health programmes can improve worker health
Since 1979 Johnson & Johnson has run a comprehensive, holistic workplace health and wellness programme. The programme integrates disability management, occupational health, employee assistance, work-life programmes, wellness, and fitness (Bartz, 2018[25]). The objective is to create an environment that fosters and supports healthy choices through fitness centres, step challenges, healthy food, a tobacco-free environment, mental well-being, weight loss programmes, and medical coverage. Participants receive a financial incentive to complete a health risk assessment followed by meetings with health advisor to develop a plan for reducing any identified risks. The programme has achieved high participation rates and has significantly reduced risk factors (such as physical inactivity, smoking, high blood pressure and cholesterol) (Goetzel et al., 2002[26]). In turn this has led to lower overall corporate health care spending, less absenteeism, and a positive return on investment. The return on investment in Johnson & Johnson’s programme has been estimated at between USD 1.88 – 3.92 for every dollar spent (Henke et al., 2011[27]). All employees have access to a course called Energy for Performance during which participants identify and prioritise the most meaningful parts of their lives. Johnson & Johnson has found this has improved productivity and increased retention (Bartz, 2018[25]).
The LifeWorks@TURCK platform is a comprehensive, integrated set of services and programmes that has developed incrementally since 2003, directed at the creation of a culture of health and well-being (Pronk, Lagerstrom and Haws, 2015[28]). Based primarily in Minneapolis, the United States, TURCK is a manufacturer of industrial automation technology. Between 2008‑10, a framework promoting five pillars of well-being (financial, social, career, physical and community) was established (Pronk, Lagerstrom and Haws, 2015[28]). Services include an on-site health clinic focused on screening for diseases such as diabetes and cancer, an on-site pharmacy, financial budget planning, 1‑on‑1 financial counselling, and a volunteering company match. The programme is embedded into the culture of the organisation and has become TURCK’s employment brand. It has had a positive impact on operating earnings, as well as retention, job satisfaction, and recruitment of new workers (Pronk, Lagerstrom and Haws, 2015[28]).
SMEs need more support in implementing workplace health promotion programmes
Large companies are more likely than small and medium-sized enterprises (SMEs) to offer health and well-being programmes. In the United States, 33% of the smallest firms (50‑100 employees) have a wellness programme, compared to 80% of the larger ones (over 1 000 employees) (OECD, 2022[29]). The barriers SMEs face in implementing WHWP include cost, the lack of sufficient human resources, and lack of knowledge about potential programmes. However, SMEs may be in a good position to adopt successful WHWP due to having less bureaucracy, easier implementation, and the potential for team bonding (OECD, 2022[29]). Governments and social partners can support SMEs in the process of implementing WHWP by strengthening occupational health services, developing national accreditation for health and well-being providers, and by creating certified recognition programmes for employers and offering subsidies to SMEs (OECD, 2022[29]). The CDC argue that workplace health promotion programmes are more likely to be successful if occupational safety and health is considered in their design and execution (Centers for Disease Control and Prevention, 2016[24]). An example of a certified recognition programme is the Health and Productivity Management (H&PM) programme in Japan (Box 3.3).
Box 3.3. Health and Productivity Management Programme (H&PM) in Japan
In Japan the Health and Productivity Management Programme (H&PM) provides both certification and awards for employers who take measures to promote health and well-being at the workplace, and also aims to incentivise investment in such health-promoting corporations. Whereas large corporations are required to fill in a dedicated H&PM questionnaire, SMEs only need to submit written evidence for assessment, given that the questionnaire requires detailed information that may not be collected regularly by smaller companies. The top 500 SMEs are awarded “Bright 500” status and the top 500 large corporations are awarded “White 500 Corporation” status.
High-performing companies have lower rates of smoking, hypertension (high blood pressure) and hyperglycaemia (high blood pressure) among other outcomes. There are also significant monetary benefits for employers. Employer medical expenditure for employee health is considerably lower in higher-performing companies, and turnover rates (5.4%) in the top-performers were about half of the turnover rates in companies across Japan (11.4%), suggesting that H&PM implementation enhances employee retention and loyalty. Large corporations also receive an individualised feedback sheet based on their responses to the H&PM survey that helps them to diagnose areas for improvement.
Source: OECD (2022[29]), Promoting Health and Well-being at Work: Policy and Practices, https://doi.org/10.1787/e179b2a5-en.
3.2.2. Redesigning the workplace to prevent poor health outcomes
The Work and Well-Being Initiative, a joint Harvard and MIT research-for-action initiative has proposed a toolkit designed to help reshape work conditions that are a root cause of stress-related health problems. The toolkit is based on three principles: i) increasing worker schedule control and voice, ii) moderating job demands, and iii) providing training and employer support aimed at enhancing social relations at work (Lovejoy et al., 2021[30]; The Work and Well-Being Initiative, 2021[31]). This toolkit has been established in response to the often‑poor effectiveness of corporate health and well-being programmes, however there are some similarities with the promising practices for WHWP discussed above.
Control at work involves having meaningful discretion over how, when, and where work gets done (Kelly and Moen, 2020[32]). A lack of control over important aspects of work life can be stressful, particularly combined with high work demands. Working time autonomy has been shown to improve productivity and reduce labour turnover (Moen, Kelly and Hill, 2011[33]; Beckmann, Cornelissen and Kräkel, 2017[34]; Shepard, Clifton and Kruse, 1996[35]). A work design initiative called STAR (Support. Transform. Achieve. Results.) implemented in a Fortune 500 company made three changes to reduce employee burnout (Kelly et al., 2014[36]). Employees were given greater control over when and where they work. Managers were trained to focus on “results” rather than “face‑time” and encouraged to share their support for and interest in employees’ personal and family lives. The programme brought benefits to employees and the company. Staff were less stressed, and with fewer interruptions better able to concentrate and innovate. Better control over their schedules allowed workers to juggle work and their personal lives more effectively which benefitted physical health.
Chronic work stress is often associated with long working hours and/or work under intense pressure (Box 3.4). This affects employee’s health as well as affecting productivity by reducing employees’ ability to sleep, concentrate, make decisions well and function optimally (The Work and Well-Being Initiative, 2021[31]). When demands are excessive or are not matched with supportive conditions and resources then this contributes to excessive job strain (Box 3.1). The Work and Wellbeing Initiative shows that the management strategy known as kaizen has the potential to reduce work demands by streamlining work procedures in a participatory way. A study of Danish postal workers found that kaizen resulted in higher employee job satisfaction and better mental health (von Thiele Schwarz et al., 2017[37]).
Preventing physical strain is another key dimension to reducing workplace stress. Toolkits and other approaches can be used to undertake systematic and regular workplace risk assessments which can be used to make adaptations or adjustments to behaviour or environment to prevent health problems (Bevan and Cooper, 2022[17]). A new generation of risk assessments methods recognise that workplace, clinical and psychosocial factors can interact to generate ‘hazardous personal states’ (Bevan and Cooper, 2022[17]).4 Therefore policies need to address both physical factors such as ergonomic changes in addition to stress responses that might cause mental health problems (Bevan and Cooper, 2022[17]).
Box 3.4. Did you know? Despite regulation, excessively long working hours remain relatively widespread
Regulations on working hours vary across the OECD, but most countries set regulations on statutory normal working hours, which is supplemented by a statutory limit on maximum working hours including overtime (OECD, 2021[38]). The ILO has recently reported that in many cases there has been insufficient resources dedicated to tackling violations of working time regulations (ILO, 2018[39]). Long hours spent in paid work can impinge on leisure time, personal care, and a person’s ability to contribute to unpaid work (such as housework and caring for family members) within a household. On average, around 7% of employees in OECD countries routinely work 50 hours or more each week. The EU’s Working Time Directive requires that average weekly working hours must not exceed 48 hours including overtime. Both Japan and Korea have implemented reforms to reduce the incidence of excessively long working hours in recent years, but the statutory limit remains 51.25 hours in Japan and 52 hours in Korea. It is recognised in both Korea and Japan that excessively long working hours carry significant health costs that require policy attention (Hijzen and Thewissen, 2020[40]).
Finally, the third principle of the Work and Well-Being Initiative highlights the importance of social relationships in the workplace for employee health and well-being. Positive social connections such as supportive interactions, a sense of belonging, and effective teamwork, improve worker well-being and can prevent the harmful effects of stress (The Work and Well-Being Initiative, 2021[31]). These connections can also improve worker performance and reduce sickness absence and the likelihood of quitting. The Availability, Responsiveness, and Continuity initiative was tested among social services workers in child welfare and mental health programmes (Glisson, Dukes and Green, 2006[41]; Glisson et al., 2012[42]). This initiative provided workshops and training to improve workers’ communication, trust, and goal alignment within teams. Teams also worked together to make changes they thought would improve client services and their own experiences on the job. The initiative led to significant improvements in workplace climate and employee well-being, including reduced symptoms of employee burnout and turnover, and enhanced morale, job satisfaction, and organisational commitment.
3.2.3. Tax credits and subsidies can be used to encourage employers to invest in workplace health and well-being
There is growing appetite among governments to use tax credits and subsidies to encourage employers to invest in workplace health and well-being. For example, France, Germany, Italy and the United Kingdom all provide tax credits at the national level related to health and well-being and several others have measures at the sub-national level (Australia and the United States). In Germany, a tax exemption introduced in 2008 provides employers with an exemption for health and well-being expenditures up to EUR 600 (USD 710) per employee per year (OECD, 2022[29]). In France and the United Kingdom tax exemptions have been introduced to encourage cycling to work. In France, employers can pay employees up to EUR 500 (USD 592) per year for commuting by bicycle or car-sharing schemes as part of the Sustainability Mobility Package (Forfait Mobilité Durable) (OECD, 2022[29]).
3.2.4. Paid sick leave plays a vital role in preventing ill-health in the workplace and return to work
Preventing avoidable5 sickness absence from work due to ill-health is key to promoting health and well‑being at the workplace. Prevention policies can also play a key role later in life in conjunction with government polices such as paid sick leave. Sick leave can allow sick workers to recover at home and ensure that they have access to medical support. However, long-term absence from work due to sickness can also have long lasting effects on labour market outcomes. The COVID‑19 pandemic led many OECD countries to strengthen arrangements to provide paid sick leave, and the spotlight on access to paid sick leave has led some countries to make long-term changes – placing greater emphasis on incentives for employers to prevent sick leave. Most OECD countries have a combination of employer-paid sick leave and government sickness benefit for workers on sickness absence, Japan, Korea and the United States being the exceptions.
The period and replacement rate of sick leave is particularly important as it has the potential to create a financial incentive for employers to promote better health among their employees, but in most countries the duration of employer-paid sick leave tends to be too short to provide a strong incentive to reduce or prevent sickness absence (OECD, forthcoming[43]; 2022[29]). Paid sick leave replaces on average, 65% of an eligible employee’s wage during a two‑week sickness spell. In some countries, such as Ireland, the United Kingdom, the United States and Korea, some workers may receive non-mandatory sick pay from their employer (OECD, forthcoming[43]).
3.2.5. Promote timely return-to-work and workplace accommodations
Governments should promote recovery and return-to-work of partially recovered workers early on during a sickness absence to avoid the prospect of paid sick leave becoming an exit route out of the labour force. Evidence from several OECD countries, including Belgium, the Netherlands, and the United Kingdom, shows that return-to-work becomes increasingly difficult as the duration of absence lengthens, particularly after three months of absence (OECD, 2015[44]). In the Netherlands, employees and employers have strong incentives to do everything they can to reintegrate sick employers, including offering retraining (OECD, forthcoming[43]). In Korea a return-to-work programme called My job, Tomorrow Service provides integrated medical, psychological care and vocational rehabilitation services for employees with a disability due to an accident or occupational injury (OECD, forthcoming[43]). Making substantial changes to a production process to improve the match between worker abilities and job demands can also yield positive results (Box 3.5).
Capacity-oriented sickness certificates like those used in Denmark, the Netherlands and Norway can be used to promote recovery by showing what work and tasks a sick worker can still reasonably do and what accommodation is necessary (OECD, forthcoming[43]). Work capacity should be regularly reassessed by all actors involved as these are an efficient way to reduce sickness absence and promote return-to-work. Reassessment six months into the sick leave spell reduced the time until partial or full work could be resumed by approximately 20 days in Norway (Markussen, Røed and Schreiner, 2018[45]).
Box 3.5. Adapting workplaces to retain older workers – the Ford Fiesta production line in Cologne
To develop a new production process at the Ford Fiesta factory in Cologne, it was necessary to close an in-house manufacturing plant affecting 5 000 employees, including 500, mainly older workers with acquired disabilities. For health reasons these workers could only carry out simple assembly jobs. Ford and the Institute for Quality Assurance in Prevention and Rehabilitation (IQPR) in Cologne used innovative methods to re‑integrate workers with acquired disabilities (mainly musculoskeletal diseases and cardiovascular diseases) into the new manufacturing process. An interdisciplinary integration team was formed which used software to match the demands of a job with the precise abilities of a particular worker. The ability profiles were prepared by physicians, with the employee’s consent.
Over 300 workers were re‑integrated into production jobs which brought about huge economic advantages including saving recruitment costs of up to USD 9 million per year. Rates of sickness absence also fell from over 20% to about 7% due to improved job satisfaction and motivation. Disability rates also fell as job demands were reduced or adjusted to the specific needs of employees. The project also brought about long-term change – the move from a “deficit-oriented approach”, with the focus on what an employee can no longer do, to a “resource‑oriented approach”.
Source: Eurofound (2005[46]), Ford Werke, Germany: Redeployment, health and well-being, https://www.eurofound.europa.eu/observatories/eurwork/case-studies/ageing-workforce/ford-werke-germany-redeployment-health-and-well-being.
In most OECD countries, employers are obliged to make adjustments for workers with disabilities, but often this does not extend to workers experiencing sickness, illness or injury (OECD, 2022[29]). Expanding eligibility to workers with health conditions would be beneficial, particularly for older workers. Accommodation costs are often minimal, as it usually involves an increase in flexibility for employees rather than an increase in expenditure (OECD, 2021[47]).
Graded work facilitates a gradual return to work allowing workers to return to work sooner, perhaps working different, lighter duties, which prevents the loss of skills and experience and can be helpful for rehabilitation from some diseases (Kools and Koning, 2019[48]). Many European OECD countries facilitate gradual return-to-work by allowing workers to continue to receive a proportion of paid sick leave (OECD, forthcoming[43]). Evidence from Germany suggests that the use of gradual return-to-work reduces the duration of sickness absence and reduces the risk of labour market exit into disability benefits (Schneider, Linder and Verheyen, 2016[49]).
3.2.6. Adapt workplace policies to promote positive mental health
Many of the risk factors associated with poor mental health such as unemployment, fear and financial insecurity reached new heights amidst the COVID‑19 pandemic. In some countries the prevalence of anxiety in early 2020 was double or more than double the level observed in previous years (OECD, 2021[50]). Although many governments and employers have reacted rapidly to scale up mental health services, the scale of the mental distress since the start of the pandemic requires more integrated, whole‑of-society mental health support (OECD, 2021[50]).
Employers play an important role in helping their employees manage and deal with mental health issues, yet there remains a lack of awareness and understanding of the impact mental health can have on individuals and the labour productivity losses that can result from poor mental health among employees. Psychosocial risks should be a core component of occupational health and safety policies. The 2022 AARP Global Employee Survey found that in most of the 12 countries in the survey, mature workers are less likely to agree or strongly agree that their employer promotes mental and/or physical health compared to younger workers (Figure 3.4). This suggests that there is significant potential to improve the promotion of mental and physical health in workplaces, particularly in Korea, Japan, Spain and Italy, where levels of employee agreement are quite low.
Figure 3.4. Mature workers are less likely to agree that their employer promotes mental and/or physical health compared to younger workers
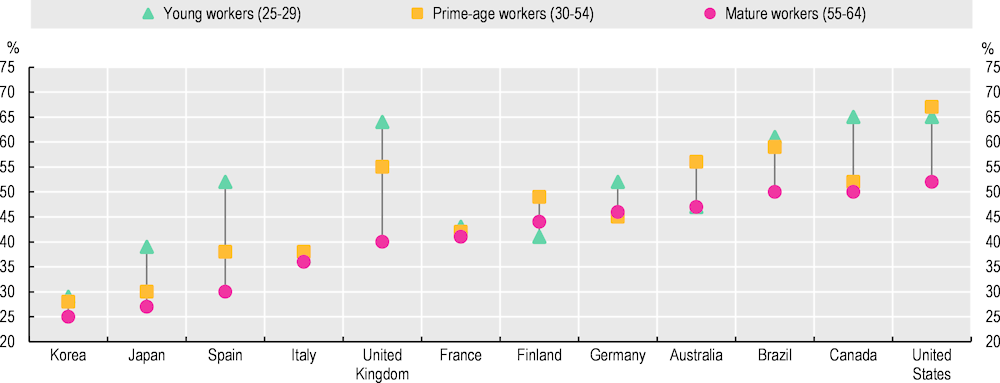
Note: Persons who replied “agree or strongly agree” to the question “My employer promotes mental and/or physical health”.
Source: AARP Global Employee Survey. Online survey conducted in June/July 2022 of employees aged 25 and over in the 12 countries shown. Approximately 1 000 respondents in each country.
Employers can take proactive steps to promote and provide mental health support to all employees Box 3.6. Effective approaches include tackling stigma at work, encouraging the disclosure of mental health problems among employees as well as practical tools for employees to monitor their stress levels and face‑to-face counselling. The OECD Recommendation on Integrated Mental Health, Skills and Work Policy (2015[51]), adopted by all OECD members in 2015, calls for policies to promote psychosocial risk assessment, to increase awareness and competence of line managers in mental health, and to support return-to-work for workers experiencing mental health issues on sick leave.
Box 3.6. Promoting mental health in the workplace
Bell Canada is a telecommunications company with over 52 000 employees. In 2010, the company launched the “Let’s talk” initiative to focus on the mental health of its work force. The programme includes enhanced access to care, as well as practices to remove stigma from mental health issues in the workplace, such as the creation of a brochure on communication with fellow employees who might be struggling, as well as a toolkit, proposing self-care activities to employees and providing a forum for discussion. The initiative also offers an enhanced return to work programme as well as mandatory leader training on mental health issues. Since 2011, the “Let’s talk” fund has provided more than 1 000 grants to organisations promoting mental health (Bell Canada, 2022[52]). The return on investment has consistently been positive, with an estimated return of CAD 4.1 for every Canadian dollar invested in the programme. Other KPIs have also shown positive change, with use of the Employee and Family Assistance Program (EFAP) being double that of the industry and national standard, short-term disability claims decreasing by 20% and mental health related short-term disability recurrence dropping by 50% since the launch of the programme in 2010 (Deloitte, 2019[53]).
In Japan, SMEs implementing a Mental Health Promotion Plan can apply for a subsidy of up to JPY 100 000 (USD 911). Since 2015, subsidies have been provided to all employers in Japan with more than 50 employees to offer a required stress check to their employees (OECD, 2022[29]).
In the United Kingdom the mental health charity Mind developed a guide for employers on how to meet and implement the six core standards for mental health in the workplace (Stevenson and Farmer, 2017[54]). A toolkit is available on how to implement the Thriving at Work standards in the workplace (Farmer, 2018[55]). The core standards include: i) develop mental health awareness among employees by making information, tools and support accessible, ii) encourage open conversations about mental health and the support available when employees are struggling, during the recruitment process and at regular intervals throughout employment, and iii) provide employees with good working conditions and ensure they have a healthy work/life balance and opportunities for development (Farmer, 2018[55]).
New working practices such as telework demand new protections for workers’ mental health
Telework can increase the risks of working long hours and burnout. Evidence from before the COVID‑19 crisis on the interaction between teleworking and mental health was mixed (OECD, 2021[12]), and the take‑up of teleworking in OECD countries was limited before the pandemic.6 Telework offers benefits such as flexible working arrangements, elimination of commuting time, and the possibility to better balance work and family commitments. However, telework can also blur the boundaries between work and home, increase usage of digital technologies, and contribute to extended working hours, and result in a sense of detachment from the workplace, all of which can have a negative impact on mental health (OECD, 2021[12]).
Spurred on by the rise in telework amidst the COVID‑19 crisis, policy makers are already making attempts to deal with the negative mental health impacts of the digital transformation of the workplace. New regulations around teleworking may also be required to protect workers’ mental health, and policy makers have already responded rapidly in several countries in this area. Some countries, including France, Italy, Spain and Luxembourg, Greece and the Slovak Republic, now have legislation in place giving workers the right to digitally disconnect from work outside of standard working hours (Eurofound, Weber and Vargas Llave, 2021[56]).
References
[18] Baicker, K., D. Cutler and Z. Song (2010), “Workplace Wellness Programs Can Generate Savings”, Health Affairs, Vol. 29/2, https://doi.org/10.1377/hlthaff.2009.0626.
[25] Bartz, A. (2018), This Healthcare Company Is Determined to Have the Healthiest Employees in the World, https://www.jnj.com/innovation/how-johnson-johnson-is-improving-workplace-wellness-for-healthiest-employees (accessed on 2 December 2022).
[19] Baxter, S. et al. (2014), “The relationship between return on investment and quality of study methodology in workplace health promotion programs”, American Journal of Health Promotion, Vol. 28/6, pp. 347-363, https://doi.org/10.4278/ajhp.130731-LIT-395.
[34] Beckmann, M., T. Cornelissen and M. Kräkel (2017), “Self-managed working time and employee effort: Theory and evidence”, Journal of Economic Behavior & Organization, Vol. 133, pp. 285-302, https://doi.org/10.1016/J.JEBO.2016.11.013.
[52] Bell Canada (2022), Bell Let’s Talk, https://letstalk.bell.ca/en/ (accessed on 21 November 2022).
[17] Bevan, S. and C. Cooper (2022), The Healthy Workforce. Enhancing Wellbeing and Productivity in the Workers of the Future, Emerald Publishing, Bingley.
[7] Cazes, S., A. Hijzen and A. Saint-Martin (2015), “Measuring and Assessing Job Quality: The OECD Job Quality Framework”, OECD Social, Employment and Migration Working Papers, No. 174, OECD Publishing, Paris, https://doi.org/10.1787/5jrp02kjw1mr-en.
[24] Centers for Disease Control and Prevention (2016), Workplace Health Model, https://www.cdc.gov/workplacehealthpromotion/model/index.html (accessed on 12 December 2022).
[20] Chapman, L. (2012), “Meta-Evaluation of Worksite Health Promotion Economic Return Studies: 2012 Update”, American Journal of Health Promotion, Vol. 26/4, https://doi.org/10.4278/AJHP.26.4.TAHP.
[6] Cottini, E. and C. Lucifora (2013), “Mental Health and Working Conditions in Europe:”, https://doi.org/10.1177/001979391306600409, Vol. 66/4, pp. 958-988, https://doi.org/10.1177/001979391306600409.
[53] Deloitte (2019), The ROI in workplace mental health programs: Good for people, good for business, https://www2.deloitte.com/us/en/insights/topics/talent/workplace-mental-health-programs-worker-productivity.html (accessed on 21 November 2022).
[46] Eurofound (2005), Ford Werke, Germany: Redeployment, health and well-being, https://www.eurofound.europa.eu/observatories/eurwork/case-studies/ageing-workforce/ford-werke-germany-redeployment-health-and-well-being (accessed on 6 December 2022).
[56] Eurofound, T. Weber and O. Vargas Llave (2021), Right to disconnect: exploring company practices, Publications Office of the European Union, https://data.europa.eu/doi/10.2806/748556 (accessed on 5 September 2022).
[55] Farmer, P. (2018), How to implement the Thriving at Work mental health standards in your workplace, https://www.mind.org.uk/media-a/5762/mind_taw_a4_report_july18_final_webv2.pdf (accessed on 6 December 2022).
[41] Glisson, C., D. Dukes and P. Green (2006), “The effects of the ARC organizational intervention on caseworker turnover, climate, and culture in children’s service systems”, Child Abuse & Neglect, Vol. 30/8, pp. 855-880, https://doi.org/10.1016/J.CHIABU.2005.12.010.
[42] Glisson, C. et al. (2012), “Randomized Trial of the Availability, Responsiveness, and Continuity (ARC) Organizational Intervention With Community-based Mental Health Programs and Clinicians Serving Youth”, Journal of the American Academy of Child & Adolescent Psychiatry, Vol. 51/8, pp. 780-787, https://doi.org/10.1016/J.JAAC.2012.05.010.
[23] Goetzel, R. and R. Ozminkowski (2008), “The Health and Cost Benefits of Work Site Health-Promotion Programs”, Annual Review of Public Health, Vol. 29, pp. 303-323, https://doi.org/10.1146/ANNUREV.PUBLHEALTH.29.020907.090930.
[26] Goetzel, R. et al. (2002), “The Long-Term Impact of Johnson & Johnson’s Health & Wellness Program on Employee Health Risks”, Journal of Occupational and Environmental Medicine, Vol. 44/5, pp. 417-424.
[13] Haskel, J. and J. Martin (2022), “Economic inactivity and the labour market experience of the long-term sick”, https://www.imperial.ac.uk/people/j.haskel/document/9802/Haskel%20Martin%20sickness%20inactivity%20v2/?Haskel%20Martin%20sickness%20inactivity%20v2.pdf (accessed on 21 September 2022).
[27] Henke, R. et al. (2011), “Recent experience in health promotion at Johnson & Johnson: Lower health spending, strong return on investment”, Health Affairs, Vol. 30/3, pp. 490-499, https://doi.org/10.1377/HLTHAFF.2010.0806/ASSET/IMAGES/LARGE/2010.0806FIGEX2.JPEG.
{kind=link}
[40] Hijzen, A. and S. Thewissen (2020), “The 2018-2021 working time reform in Korea: A preliminary assessment”, OECD Social, Employment and Migration Working Papers, No. 248, OECD Publishing, Paris, https://doi.org/10.1787/0e828066-en.
[39] ILO (2018), General Survey concerning working-time instruments - Ensuring decent working time for the future, https://www.ilo.org/ilc/ILCSessions/previous-sessions/107/reports/reports-to-the-conference/WCMS_618485/lang--en/index.htm (accessed on 25 March 2022).
[32] Kelly, E. and P. Moen (2020), Overload: How Good Jobs Went Bad and What We Can Do About It, Princeton University Press, Princeton, NJ.
[36] Kelly, E. et al. (2014), “Changing Work and Work-Family Conflict”, American Sociological Review, Vol. 79/3, pp. 485-516, https://doi.org/10.1177/0003122414531435.
[48] Kools, L. and P. Koning (2019), “Graded return-to-work as a stepping stone to full work resumption”, Journal of Health Economics, Vol. 65, pp. 189-209, https://doi.org/10.1016/J.JHEALECO.2019.03.009.
[30] Lovejoy, M. et al. (2021), “Work Redesign for the 21st Century: Promising Strategies for Enhancing Worker Well-Being”, American Journal of Public Health, Vol. 111/10, pp. 1787-1795, https://doi.org/10.2105/AJPH.2021.306283.
[45] Markussen, S., K. Røed and R. Schreiner (2018), “Can Compulsory Dialogues Nudge Sick-listed Workers Back to Work?”, The Economic Journal, Vol. 128/610, pp. 1276-1303, https://doi.org/10.1111/ECOJ.12468.
[5] Marmot, M. et al. (2020), Health Equity In England: The Marmot Review 10 Years On, The UCL Institute of Health Equity, London.
[10] Marmot, M. et al. (2010), Fair Society Healthy Lives (The Marmot Review), https://www.instituteofhealthequity.org/resources-reports/fair-society-healthy-lives-the-marmot-review (accessed on 7 September 2022).
[4] Marmot, M. and G. Smith (1997), “Socio-economic Differentials in Health.”, Journal of health psychology, Vol. 2/3, pp. 283-96, https://doi.org/10.1177/135910539700200302.
[21] Mattke, S. et al. (2013), “Workplace Wellness Programs Study: Final Report”, Workplace Wellness Programs Study: Final Report, https://doi.org/10.7249/RR254.
[9] McNamara, T. and H. Tinsley-Fix (2018), Creating Quality Jobs: A Framework for the Multigenerational Workforce, AARP, https://www.aarp.org/content/dam/aarp/work/employers/2019/05/creating-quality-jobs-a-framework-for-the-multigenerational-workforce-aarp-2018.pdf (accessed on 28 July 2022).
[33] Moen, P., E. Kelly and R. Hill (2011), “Does Enhancing Work-Time Control and Flexibility Reduce Turnover? A Naturally Occurring Experiment”, Social problems, Vol. 58/1, p. 69, https://doi.org/10.1525/SP.2011.58.1.69.
[57] Oakman, J. and W. Macdonald (2019), “The APHIRM toolkit: an evidence-based system for workplace MSD risk management”, BMC musculoskeletal disorders, Vol. 20/1, p. 504, https://doi.org/10.1186/S12891-019-2828-1/TABLES/3.
[16] OECD (2022), Disability, Work and Inclusion: Mainstreaming in All Policies and Practices, OECD Publishing, Paris, https://doi.org/10.1787/1eaa5e9c-en.
[29] OECD (2022), Promoting Health and Well-being at Work: Policy and Practices, OECD Health Policy Studies, OECD Publishing, Paris, https://doi.org/10.1787/e179b2a5-en.
[14] OECD (2022), Report on the Implementation of the OECD Recommendation on Ageing and Employment Policies, OECD, Paris.
[47] OECD (2021), Disability, Work and Inclusion in Ireland: Engaging and Supporting Employers, OECD Publishing, Paris, https://doi.org/10.1787/74b45baa-en.
[12] OECD (2021), Fitter Minds, Fitter Jobs: From Awareness to Change in Integrated Mental Health, Skills and Work Policies, Mental Health and Work, OECD Publishing, Paris, https://doi.org/10.1787/a0815d0f-en.
[3] OECD (2021), Health at a Glance 2021: OECD Indicators, OECD Publishing, Paris, https://doi.org/10.1787/ae3016b9-en.
[38] OECD (2021), OECD Employment Outlook 2021: Navigating the COVID-19 Crisis and Recovery, OECD Publishing, Paris, https://doi.org/10.1787/5a700c4b-en.
[50] OECD (2021), “Tackling the mental health impact of the COVID-19 crisis: An integrated, whole-of-society response”, OECD Policy Responses to Coronavirus (COVID-19), OECD Publishing, Paris, https://doi.org/10.1787/0ccafa0b-en.
[2] OECD (2020), Promoting an Age-Inclusive Workforce: Living, Learning and Earning Longer, OECD Publishing, Paris, https://doi.org/10.1787/59752153-en.
[15] OECD (2018), Ageing and Employment Policies: United States 2018: Working Better with Age and Fighting Unequal Ageing, Ageing and Employment Policies, OECD Publishing, Paris, https://doi.org/10.1787/9789264190115-en.
[44] OECD (2015), Fit Mind, Fit Job: From Evidence to Practice in Mental Health and Work, Mental Health and Work, OECD Publishing, Paris, https://doi.org/10.1787/9789264228283-en.
[51] OECD (2015), Recommendation of the Council on Integrated Mental Health, Skills and Work Policy, https://legalinstruments.oecd.org/en/instruments/OECD-LEGAL-0420.
[11] OECD (2012), Sick on the Job?: Myths and Realities about Mental Health and Work, Mental Health and Work, OECD Publishing, Paris, https://doi.org/10.1787/9789264124523-en.
[43] OECD (forthcoming), Towards equitable and adequate paid sick leave in Korea, OECD Publishing, Paris.
[28] Pronk, N., D. Lagerstrom and J. Haws (2015), “Lifeworks@turck a best practice case study on workplace well-being program design”, ACSM’s Health and Fitness Journal, Vol. 19/3, pp. 43-48, https://doi.org/10.1249/FIT.0000000000000120.
[22] Royer, H., M. Stehr and J. Sydnor (2015), “Incentives, Commitments, and Habit Formation in Exercise: Evidence from a Field Experiment with Workers at a Fortune-500 Company”, American Economic Journal: Applied Economics, Vol. 7/3, pp. 51-84, https://doi.org/10.1257/app.20130327.
[8] Saint-Martin, A., H. Inanc and C. Prinz (2018), “Job Quality, Health and Productivity: An evidence-based framework for analysis”, OECD Social, Employment and Migration Working Papers, No. 221, OECD Publishing, Paris, https://doi.org/10.1787/a8c84d91-en.
[49] Schneider, U., R. Linder and F. Verheyen (2016), “Long-term sick leave and the impact of a graded return-to-work program: evidence from Germany”, European Journal of Health Economics, Vol. 17/5, pp. 629-643, https://doi.org/10.1007/S10198-015-0707-8/TABLES/4.
[35] Shepard, E., T. Clifton and D. Kruse (1996), “Flexible Work Hours and Productivity: Some Evidence from the Pharmaceutical Industry”, Industrial Relations: A Journal of Economy and Society, Vol. 35/1, pp. 123-139, https://doi.org/10.1111/J.1468-232X.1996.TB00398.X.
[54] Stevenson, D. and P. Farmer (2017), Thriving at work, Department for Work and Pensions and Department of Health and Social Care, https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/658145/thriving-at-work-stevenson-farmer-review.pdf (accessed on 6 December 2022).
[31] The Work and Well-Being Initiative (2021), Employer Toolkit: Work Design for Health, https://workwellbeinginitiative.org/employertoolkit (accessed on 7 December 2022).
[37] von Thiele Schwarz, U. et al. (2017), “Using kaizen to improve employee well-being: Results from two organizational intervention studies”, Human Relations, Vol. 70/8, pp. 966-993, https://doi.org/10.1177/0018726716677071.
[1] Webber, D. et al. (2015), Does poor health affect employment transitions?, Joseph Rowntree Foundation, York, https://www.jrf.org.uk/report/does-poor-health-affect-employment-transitions (accessed on 29 November 2022).
Notes
← 1. The terms “mature” and “older” are used interchangeably throughout this report.
← 2. In 2016‑19, the disability employment gap, measured as the difference in the employment rate between people without a disability and people with a disability, was 27 percentage points on average across 32 OECD countries, ranging from around 15 percentage points in Mexico, Chile and Switzerland to over 35 percentage points in Lithuania, the United States and Ireland (OECD, 2022[16]).
← 3. In the studies reviewed by Baicker, Cutler and Song (2010[18]) programmes included a health risk assessment in 81% of firms. In 42% of firms self-help education materials where included, individual counselling was available in 39% of firms, classes, seminars, and group activities were available in 36%, and additional incentives for participation were included in 31% of firms.
← 4. For example the risk assessment model of Oakman and Macdonald (2019[57]).
← 5. Illnesses that are at least partly caused by modifiable health risk factors and poor lifestyle habits.
← 6. In the EU in 2015, according to European Working Conditions Survey data, only 3% of employees regularly worked from home, a further 5% “highly mobile” employees worked regularly from several locations (including home), and another 10% of workers occasionally worked from home (OECD, 2021[38]).