This Annex summarises (1) the results of the questionnaire on care recipients and (2) the findings of the focus groups on co-ordination with health care professionals. It describes the socio-economic situation, the LTC needs of care recipients and their access to aids. Then, it provides insights on the challenges faced in care co-ordination with health care professionals.
Improving Long-Term Care in Croatia
OECD Health Policy Studies

Annex B. The profile of care recipients
Two-thirds of care recipients are poor older women, living with others
Two-thirds of care recipients are women, of whom over two-thirds are aged eighty or over. About 83% have at least one child and among them 61% live with at least one of them. In other words, half of care recipients live with at least one of their children. About 15% of care recipients live alone, 40% live with someone else and 22% with two other people or more.
Care recipients aged between 65 and 79 are concentrated mostly in northern counties (Bjelovar-Bilogora, Koprivnica-Križevci, Sisak-Moslavina, Virovitica-Podravina, Varaždin and Krapina-Zagorje) (Figure A B.1). However, this does not mean that they are in better health than in other countries. The share of care recipients in poor or fair health and with chronic illness is similar in all counties. Rather, these results suggest that the older people living in the northern counties become in poor health earlier than in the rest of the country.
Figure A B.1. Care recipients aged under eighty are concentrated in the northern counties
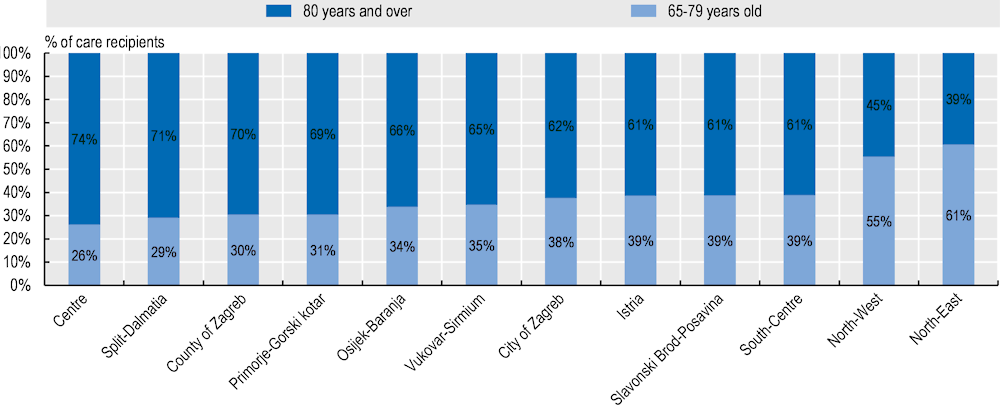
Note: Counties were grouped together when there were too few observations (<59 observations). The North-East refers to Bjelovar-Bilogora, Koprivnica-Križevci, Sisak-Moslavina and Virovitica-Podravina. The North-West refers to Varaždin and Krapina-Zagorje. The Centre refers to Karlovac and Sisak-Moslavina. The South-Centre refers to Zadar and Šibenik-Knin.
Source: OECD 2020 questionnaire to visiting nurses and carers in Croatia (visiting nurses completed this section of the questionnaire).
Over half of household of care recipients make less than HRK 4 000 every month (Figure A B.2). In comparison, the monthly minimum wage was HRK 3 750 and the median equivalised net income was HRK 4 517 in 2019. Almost one-fifth have a household income of less than HRK 2000. However, it is worth noting that visiting nurses did not provide information on income for 22% of care recipients.
Figure A B.2. Over half of households earn less than HRK 4 000 every month
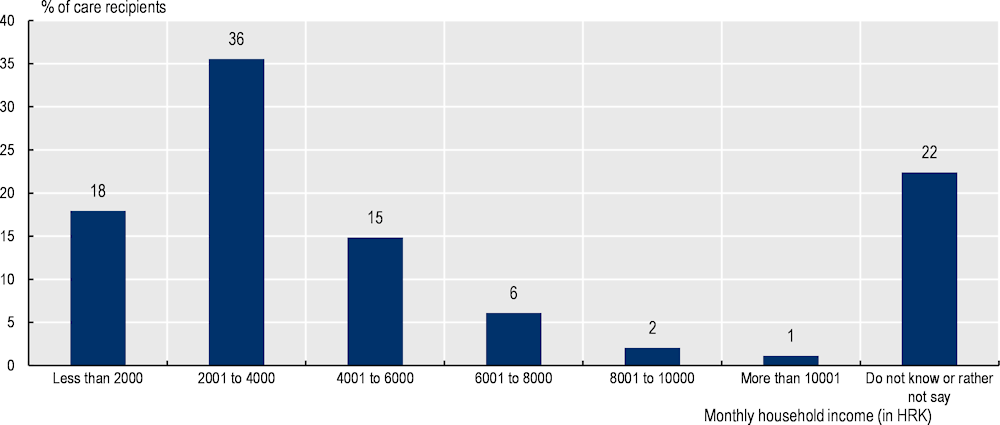
Source: OECD 2020 questionnaire to visiting nurses and carers in Croatia (visiting nurses completed this section of the questionnaire).
According to visiting nurses, about two-thirds of care recipients do not receive any of the six following benefits from social services: the help and care allowance, the personal disability allowance, the in-kind support at home, the guaranteed minimum benefit, the lump sum benefit and the compensation for housing costs (Figure A B.3). This suggests that there is room to increase the coverage of cash benefits.
Figure A B.3. About two-thirds of care recipients do not receive any of the six social benefits
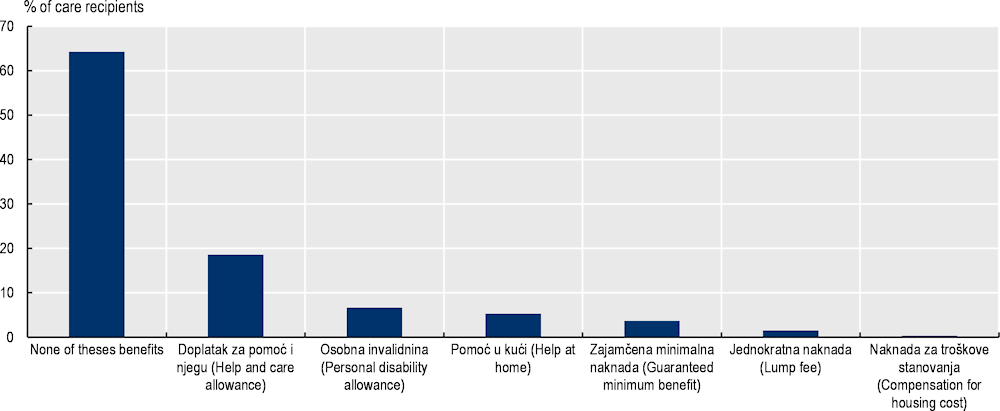
Source: OECD 2020 questionnaire to visiting nurses and carers in Croatia (visiting nurses completed this section of the questionnaire).
According to visiting nurses, almost two-thirds of care recipients own their dwelling without mortgage, while 35% report living with relatives. Less than 2% of care recipients rent their apartment.
About 88% of care recipients need major support to perform at least one ADL or IADL. About 57% of care recipients need major support to perform at least one ADL and about one-fifth of care recipients are severely limited in the five ADLs. Visiting nurses believe that 64% of care recipients could not live alone, while 31% could live alone if they receive support and only 5% could live alone independently.
Access to aids is not regarded as an issue in general, but it may be complicated in specific cases
According to visiting nurses, only 16% of care recipients do not use aids that they need on average (Figure A B.4). The rate ranges from 1% for buggies and electric wheelchair to 21% for personal alarms. The most used aids are incontinence pads, cane or walking stick, followed by walkers, raised toilet seat and manual wheelchairs.
Focus groups participants believe that procedures could be simplified to obtain certain medical aids. For instance, family carers mention that they cannot access special anti-pressure ulcer pillow through HZZO – even diagnosis of fourth-degree pressure ulcer is not considered severe enough if it is not located on certain parts of the body. They also believe that free diapers should be automatically in the list of aids of HZZO when care recipients are over a certain age (e.g. 90 years old).
Figure A B.4. Only 16% of care recipients do not use aids that they need on average
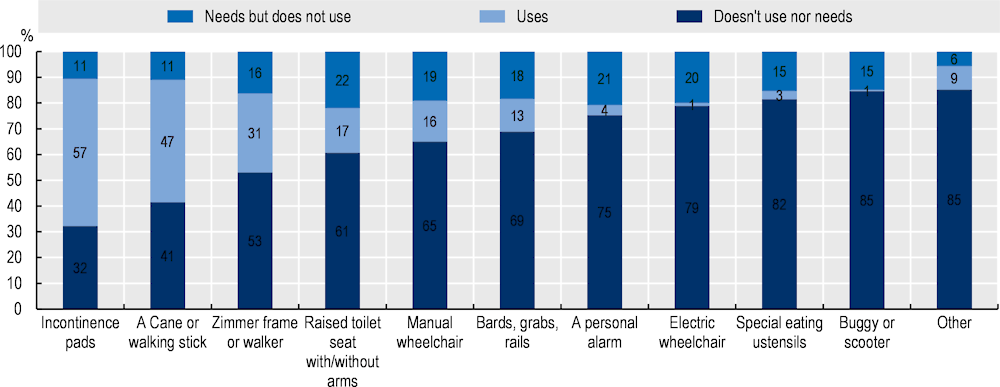
Source: OECD 2020 questionnaire to visiting nurses and carers in Croatia (visiting nurses completed this section of the questionnaire).
Co‑ordination with the health care professionals could improve according to the focus group discussions
The eleven family carers interviewed report issues related to co‑ordination with home care professionals. According to them, visiting nurses and home healthcare workers come from about once a month to a few times a week if the care recipient is immobile or with dementia. However, when the care recipient is severely dependent, they think that formal care is insufficient. In addition, visiting nurses and home healthcare workers usually come only in the morning. This means that family carers must provide similar care in the afternoon and the evening.
Doctors decide on the frequency of home visits. Receiving more support depends on visiting nurses good will to co‑ordinate with family doctors. Focus group participants also mention that doctors do not always consider visiting nurses’ suggestions, even though they are more often in contact with care recipients.
Over two-thirds of visiting nurses report performing at least one care co‑ordination tasks among their usual activities. About 73% of visiting nurses report that they refer patients to other health professionals, even though this is not their most frequent activity. Seventy-one percent of visiting nurses report developing, supervising, and co‑ordinating care of patients in consultation with doctors, and 26% of them consider this activity as their most frequent care co‑ordination task. More generally, about 74% of nurses report doing their most frequent care co‑ordination task every day, 24% a few times a week, 1% once per week and 0.5% less often.
Focus group participants also point out that one single person could carry out care currently provided by visiting nurses, home healthcare and domestic care workers. More generally, they support the idea of some type of task-shifting to reduce care co‑ordination workload.