In addition to the share of the population entitled to core health services, the extent of healthcare coverage is defined by the range of services included in a publicly defined benefit package and the proportion of costs covered. Differences across countries in the extent of coverage can be the result of specific goods and services being included or excluded in the publicly defined benefit package (such as a particular drug or medical treatment), different cost-sharing arrangements or some services only being covered for specific population groups in a country (such as dental treatment).
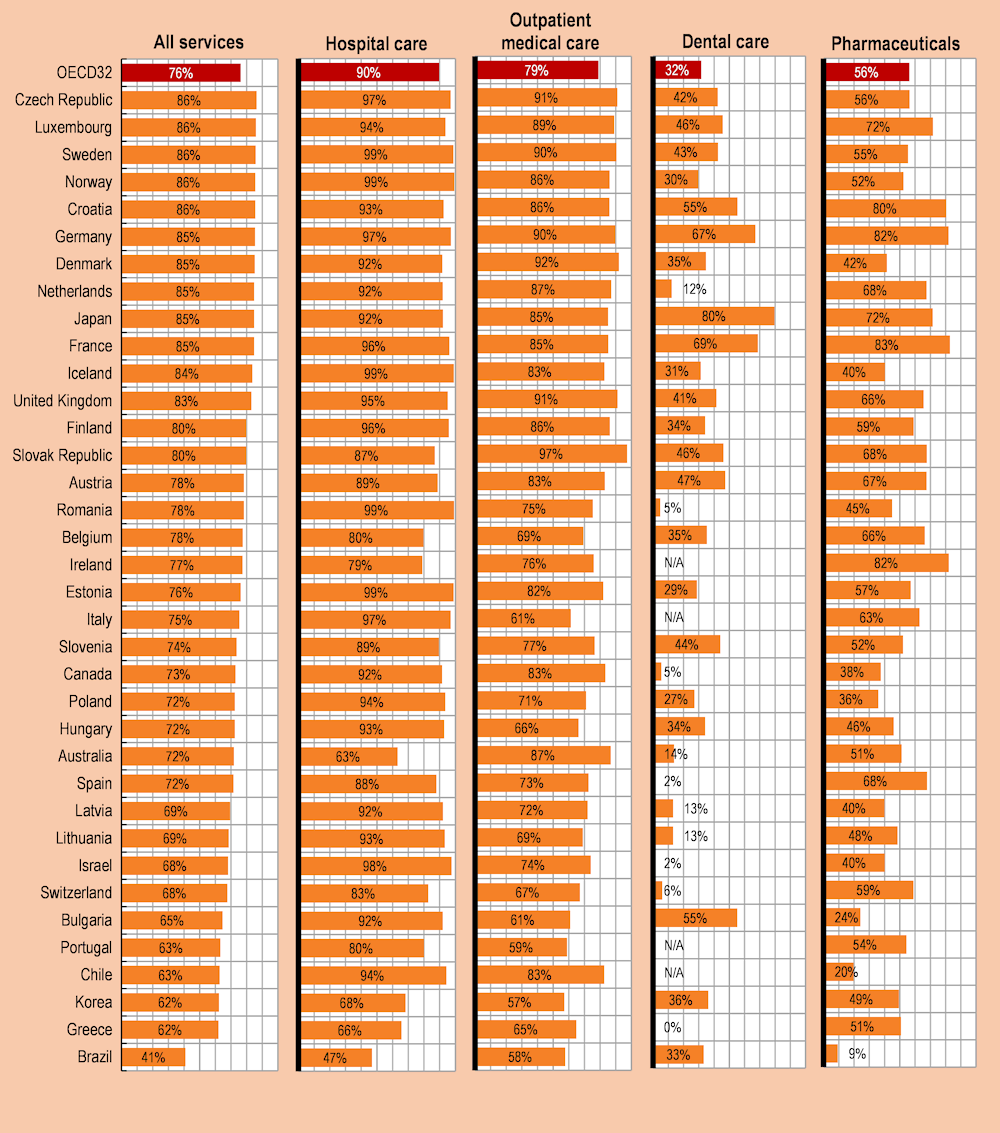
On average across OECD countries, around three‑quarters of all healthcare costs were covered by government or compulsory health insurance schemes in 2021 (see section on “Health expenditure by financing scheme” in Chapter 7), but financial protection is not uniform across all types of healthcare goods and services, and there is considerable variation across countries. In nearly all OECD countries, inpatient services in hospitals were more comprehensively covered than any other type of care, with 90% of all costs borne by government or compulsory insurance schemes in 2021 (Figure 5.7). In many countries, patients have access to free acute inpatient care or only need to make a small co-payment; as a result, coverage rates were near 100% in Sweden, Norway, Iceland and Estonia. In Australia, Greece and Korea, financial coverage for the cost of inpatient care from public sources was only around two‑thirds of total costs.
Nearly four out of every five dollars spent (79%) on outpatient medical care in OECD countries were paid by government and compulsory insurance schemes. Financial coverage ranged from under 60% in Portugal and Korea to over 90% in the Czech Republic, the Slovak Republic, Denmark and the United Kingdom. In some of these countries, outpatient primary and specialist care are generally free at the point of service, but user charges may still apply for specific services or if non-contracted private providers are consulted.
Public coverage for the cost of dental care is far more limited across OECD countries due to restricted service packages (frequently limited to children) and higher levels of cost-sharing. On average, less than one‑third of dental care costs were borne by government schemes or compulsory insurance (Figure 5.7). More than half of dental spending was covered in only three OECD countries (Japan, Germany and France), while the level of compulsory coverage was very low in Greece, Spain and Israel. Voluntary health insurance may play an important role in providing financial protection when dental care is not comprehensively covered in the benefit package – this is the case for adults in the Netherlands, for example.
Coverage for pharmaceuticals is also typically less comprehensive than for inpatient and outpatient care: across OECD countries, 56% of pharmaceutical costs were financed by government or compulsory insurance schemes. The most generous coverage was found in France (83%), Ireland (82%) and Germany (82%). On the other hand, this share was less than two‑fifths in Canada, Poland and Chile. In Canada and Poland, over one‑third of all pharmaceutical spending was financed via voluntary health insurance schemes, while in Chile, out-of-pocket payments financed nearly 80% of pharmaceutical spending (see section on “Pharmaceutical expenditure” in Chapter 9).
The COVID‑19 pandemic made apparent the impact of the degree of coverage for key health services on health systems’ resilience to shocks. Indeed, OECD countries where the entire population had health coverage for a key set of health services experienced better health outcomes (OECD, 2023[1]). During the pandemic, countries tried to ensure that diagnosis, testing and appropriate care for COVID‑19 patients were affordable – notably in countries where segments of the population remain without coverage. In Poland, for example, the National Health Fund covered uninsured as well as insured people for health services combatting COVID‑19 (OECD, 2021[2]), and in Ireland all COVID‑19‑related treatment, testing and remote GP assessments during the pandemic were available to all residents free of charge, including those who do not benefit from free regular access to GP visits (OECD/European Observatory on Health Systems and Policies, 2021[3]).