Long waiting times for elective (non-emergency) surgery have been a longstanding issue in a number of OECD countries – one that has been massively exacerbated by the COVID‑19 pandemic. By postponing the expected benefits of treatment, it means patients continue living with pain and disability for longer than they need to, and may worsen health outcomes for patients after the intervention.
Waiting times are the result of a complex interaction between the demand and supply of health services. Demand for health services and elective surgeries is determined by the health status of the population, progress in medical technologies (including the simplification of many procedures, such as cataract surgery), patient preferences and the burden of cost-sharing for patients. However, doctors play a crucial role in the decision to operate on a patient or not. On the supply side, the availability of surgeons, anaesthetists and other staff in surgical teams, as well as the supply of the required medical equipment, affects surgical activity rates.
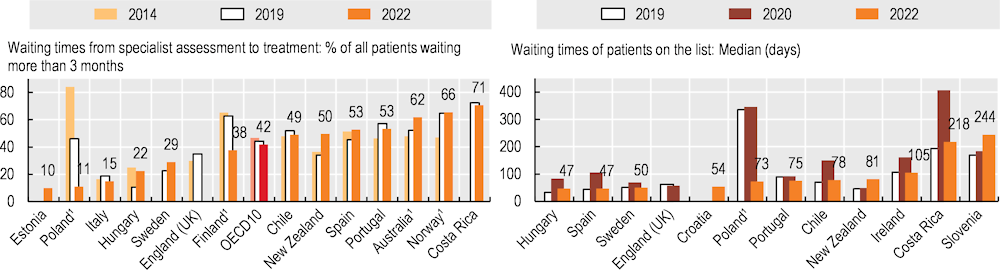
The data presented in this section focus on three high-volume surgical procedures: cataract surgery, hip replacement and knee replacement. Two measures are analysed for each surgery: the share of patients waiting more than three months from specialist assessment to treatment and the median number of days patients are on a waiting list.
Just prior to the pandemic in 2019, over 60% of patients remained on the waiting list for cataract surgery for more than three months in Costa Rica, Norway and Finland (although waiting times in Norway are overestimated compared to other countries for this and the other two surgical procedures – see the “Definition and comparability” box). The proportion of patients waiting for over three months was relatively low (20% or less) in Hungary and Italy (Figure 5.33, left panel). The median number of days a person waited was almost a year in Poland (336 days), and over 100 days in Costa Rica, Slovenia and Ireland (Figure 5.33, right panel). In the first year of the pandemic, waiting times increased in almost all countries with available data, and the median waiting time more than doubled in Costa Rica, Hungary, Spain and Chile. However, initial data for 2022 indicate that waiting times have since fallen in a number of countries, and in many countries rates are close to 2019 levels both in terms of the share of patients waiting more than three months and for median waiting times.
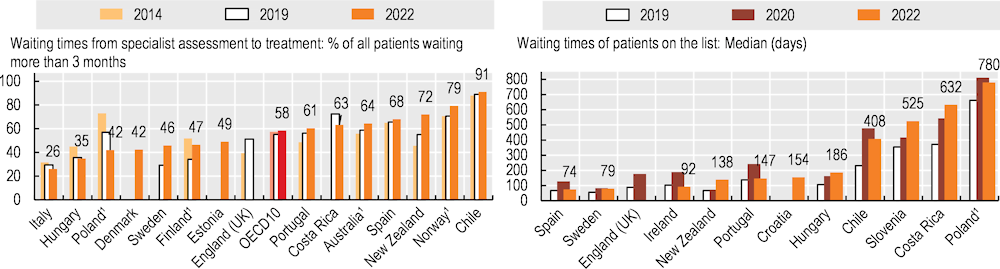
For hip replacement, the share of patients remaining on the waiting list for over three months in 2019 ranged from around 30% in Sweden and Italy, to almost 90% in Chile and over 70% in Costa Rica and Norway (Figure 5.34, left panel). The median number of days a person waited was 663 days in Poland, and around a year in Costa Rica and Slovenia (Figure 5.34, right panel). The pandemic led to waiting time increases in all countries with available data, and waiting times more than doubled in Chile and England (United Kingdom). Initial data for 2022 indicate an improved situation in most countries, but with waiting times generally still worse than in 2019, particularly in terms of median waiting times.
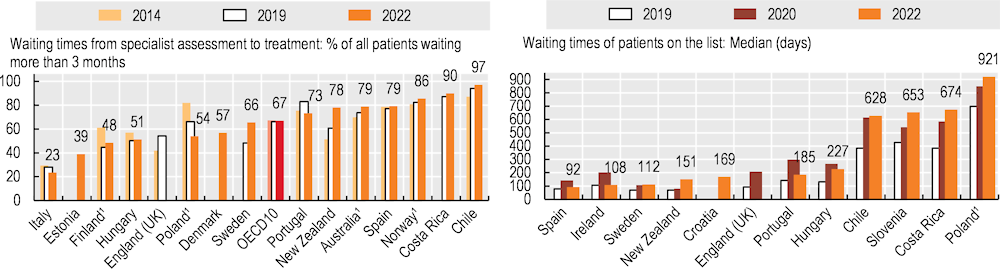
Knee replacements follow similar patterns to hip replacements (Figure 5.35, left panel). Prior to the pandemic, over 80% of patients remained on the waiting list for over three months in Chile, Costa Rica, Portugal and Norway. Median waiting times were very high in Poland, Chile, Costa Rica and Slovenia (Figure 5.35, right panel). Early in the pandemic waiting times increased in all countries with available data, although the increases were not as dramatic as for hip replacements. By 2022, waiting times had improved slightly, but were still generally worse than in 2019.
Many countries have taken actions to address the backlogs and longer waiting lists for elective care that were generated by the disruption of services during the pandemic (OECD/European Union, 2022[1]). Even prior to the pandemic, governments implemented various measures to reduce waiting times, with the most common policy being the introduction of a maximum waiting time, supported by additional funds (OECD, 2020[2]). In Poland, for example, additional funding has been provided since 2018, and information on waiting times for different procedures has become more accessible to patients through a dedicated website. These policies have contributed to some marked improvements, at least in terms of the share of people waiting for over three months from specialist assessment to treatment. More Polish people have also been purchasing private health insurance to obtain quicker access to services in private hospitals (OECD, 2020[2]).