The burden of mental illness is substantial, affecting one in two people at some point in their lives. During the COVID‑19 pandemic, levels of mental distress increased (see section on “Mental health” in Chapter 3), and the prevalence of anxiety and depression doubled in some countries (OECD, 2021[1]). The economic costs due to mental ill health have been estimated to be more than 4.2% of gross domestic product (GDP), covering both the direct costs of treatment and the indirect costs related to lower employment rates and reduced productivity (OECD, 2021[2]). High-quality, timely care has the potential to improve outcomes, and to reduce suicide and excess mortality for individuals with mental disorders.
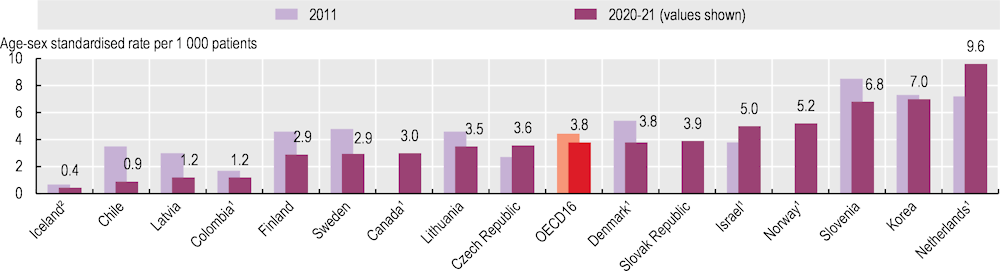
Data on quality and outcomes of care point to shortcomings in continuity of care and ongoing difficulties with improving outcomes, especially for people with severe mental disorders. Suicide rates after hospital discharge can indicate the quality of care in the community following hospitalisation, as well as co‑ordination between inpatient and community settings. Across OECD countries, suicide rates among patients who had been hospitalised in the previous year ranged from 0.4 per 1 000 patients in Iceland to almost 10 per 1 000 in the Netherlands in 2020‑21 (Figure 6.30). Differences in suicide rates may also reflect differences in access to mental health care and the severity of patient conditions that are treated in inpatient settings, as hospital discharges vary widely across countries. Between 2011 and 2021, the average suicide rate was stable across OECD countries, but there was a marked decrease in countries including Chile, Finland and Sweden. Following successful implementation of the Suicide Prevention Programme in 1992‑96, Finland introduced the National Mental Health Strategy and Suicide Prevention Agenda 2020‑30 in 2020. Korea also saw a decreased number of suicides following discharge during the pandemic.
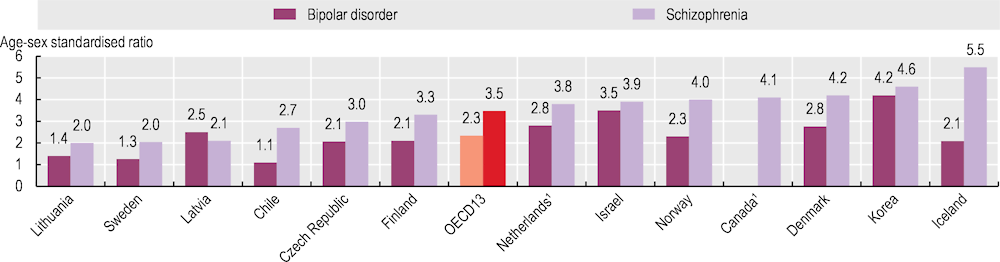
Individuals with a psychiatric illness have a higher mortality rate than the general population. An “excess mortality” value greater than one implies that people with mental disorders face a higher risk of death than the rest of the population. Figure 6.31 shows that mortality rates for people with schizophrenia and bipolar disorder are over twice as high as mortality rates for the general population in most countries. In 2021, excess mortality ranged from 2.0 in Lithuania and Sweden to 5.5 in Iceland, 4.6 in Korea 4.2 in Denmark and 4.1 in Canada for people who had lived with schizophrenia, and from 1.1 in Chile to 4.2 in Korea for people who had lived with bipolar disorders. Over the past decade, excess mortality among people with severe mental illness has increased in most countries except the Czech Republic and Sweden. Progress is notable in the Czech Republic, which started implementing mental health care strategies in 2017 focusing on providing multidisciplinary healthcare and social services to people with bipolar disorders and schizophrenia at mental health care centres in the community.
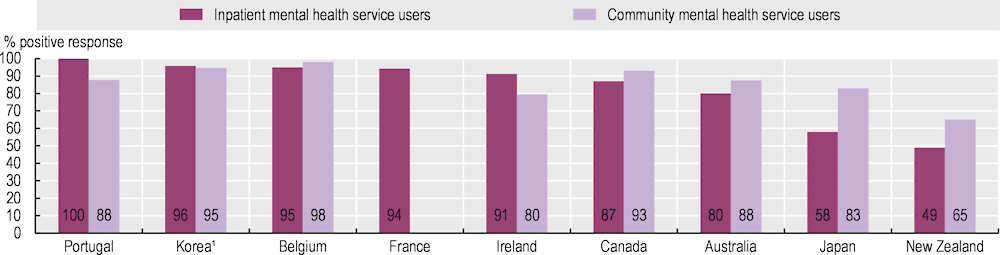
Patient-reported experience measures (PREMs) can help to capture the quality of care provided to individuals living with mental conditions. These metrics are increasingly used in mental health care to understand people’s experience of health services and to provide people‑centred mental health care (de Bienassis et al., 2021[3]; OECD, forthcoming[4]). Figure 6.32 shows service users’ perceptions of whether care providers treated them with courtesy and respect, for those in inpatient mental health settings and those using community services. The share of mental health service users reporting that they were treated with courtesy and respect in inpatient mental health services ranged from 49% in New Zealand to 100% in Portugal. In community mental health settings, the lowest share was again in New Zealand (65%), and the highest share was in Belgium (98%).